I am writing this as a sincere thank you to the Research Team and Incite Health at the Center for Primary Care at Harvard Medical School for taking the time to visit us this summer to see and hear what Direct Primary Care is all about (Here is link to story: Harvard Medical School Team Visits Gold Direct Care). If an institution of Harvard Medical Schools caliber can get behind this model of care, the potential for growth and implementation is boundless. Hopefully, we showed their team that the simplistic model of Direct Primary Care in combination with an appropriate high deductible/Health Savings Account insurance plan accomplishes everything that the Quadruple Aim is about:
Lower costs….even for insurers
Better health outcomes
Happier Doctors
All of which lead to the most important goal….HAPPIER PATIENTS!
Hopefully our relationship with their group- as well as other medical schools- will continue to grow as we continue our efforts to get more patients, doctors, employers, insurers, and legislators to buy into an old but new model of care that actually makes sense for all. The top down approach is not working so why not ground up?
So after battling with the state of Massachusetts since February, we finally got the okay to supply State Vaccines. The vaccines which we can supply are:
DTaP (Helps children develop immunity to three deadly diseases caused by bacteria: diphtheria, tetanus, and whooping cough aka pertussis.)
Hep A (Used for prevention of liver disease caused by the hepatitis A virus.)
Hep B (Used for prevention of liver disease caused by the hepatitis B virus.)
HIB (Used for prevention of invasive disease caused by Haemophilus influenzae type b bacteria.)
IPV (Used to combat poliomyelitis aka Polio.)
PCV13 (Used to protect infants and toddlers from pneumococcal disease.)
RV (Oral Dosage- Used to prevent Rotavirus which is a contagious virus that can cause gastroenteritis.)
These vaccines can be supplied to anyone under the age of 19. However, we will not be supplying HPV or Menactra(Meningococcal Meningitis Vaccine). We do have places we can send our patients to receive these vaccines at a cash price, or by using their insurance.
We will be implementing a $20 inoculation fee to help pay for the needles and syringes. This is just a one time fee per visit, NOT per vaccination.
If you have any questions, or would like to set up an appointment, please call our office at 781-842-3961.
If you would like to know more about the vaccines, or what schedule your child should be on, you can visit the CDC website here.
Thank you to Martha Bebinger from WBUR for interviewing me and publishing this great piece today on Gold Direct Care and how Direct Primary Care in general can work to improve the healthcare system as a whole. Also thank you to Mr. Bird who agreed to be interviewed that day while he was here. To reinforce why I feel the arguments against Direct Primary Care presented in the article today are weak at best:
1. DPC worsens the primary care shortage:
I ask these questions in response. What is the current system doing to fix it? Bogging down primary care doctors with more paperwork and more patients to see a day? “Value-base payments” that are based on how complex a physician “codes” their patient and visits rather than how complex the patient actually is as a human being?
By making primary care attractive to medical students from a professional and financial standpoint- including the ones I teach from Tufts Medical School- we can further supply this system with high quality, passionate students that want to do primary care for the right reason which is caring for patients. Most medical students graduate with around 150,000-250,000 dollars worth of debt. It is very challenging to offer them primary care as it currently is and currently pays. So lets fix that with Direct Primary Care.
2. DPC is “insurance”:
Without getting into legalities, the Affordable Care Act states in Section 1301 (a) (3) that Direct Primary Care combined with a catastrophic or high deductible insurance plan qualifies a patient as meeting the ACA standards of full “insurance”. However, having DPC alone would result in the patient paying the Obamacare fine. Therefore, it seems clear that DPC alone is not “insurance” or an “insurance-type product”. If you are interested in reading about this further please read this article by Dave Chase from Forbes. Mr. Chase is a great proponent of Direct Primary Care and very knowledgable on the topic.
One of the ideas which people perceive about Direct Primary Care is it’s only affordable for wealthier incomes. This article, which was well written by Marguerite Duane, MD, MHA, debunks the reasoning behind it. The link to the original article can be found at the bottom of the page.
So, if poor people have little to spend, why would the direct primary care model work for them? Simple; with direct pay models the actual health care costs can be kept much lower and therefore more affordable for these very patients. Plus, since direct pay models often have smaller patient panels, these patients may have more time with their physicians and staff to address the myriad of issues in their life that may be affecting their health.
Some direct pay models charge patients a monthly or yearly membership fee that covers all primary care office visits and even some basic or in-house labs. For example, at Qliance in Seattle, depending on the patients’ age, members pay a fee that ranges between $54 – $94 a month, which includes:
7 -day a week access to the Qliance health care team
Same or next-day appointments for urgent care
30-60 minute office visits
Phone appointments and e-visits
After hour phone access to a physician for urgent medical needs
Sure, direct primary care is great because it covers all primary care visits, but you may wonder how will poor patients pay for labs or specialty visits? It may surprise you to learn that the actual cost of most basic labs is actually very little. We negotiated with local labs to pay just above the actual cost of the tests and in exchange, we pay our lab bill in full monthly. Here is an example of how it would work for a patient with diabetes:
Labs Actual Cost Patient Paid at time of visit
HgAIC $8.72 $10
Lipid panel $3.47 $ 5
CMP $4.21 $ 5
What about the cost of specialty care, clearly this is much too expensive for poor people to afford, right? My response to that question is two-fold:
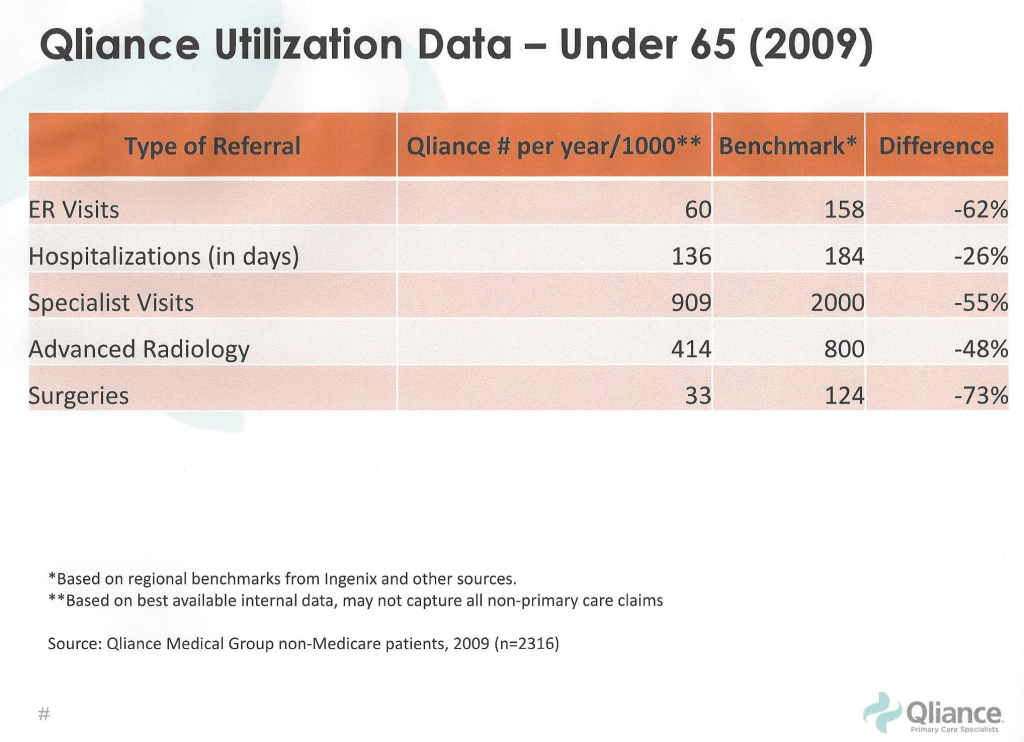
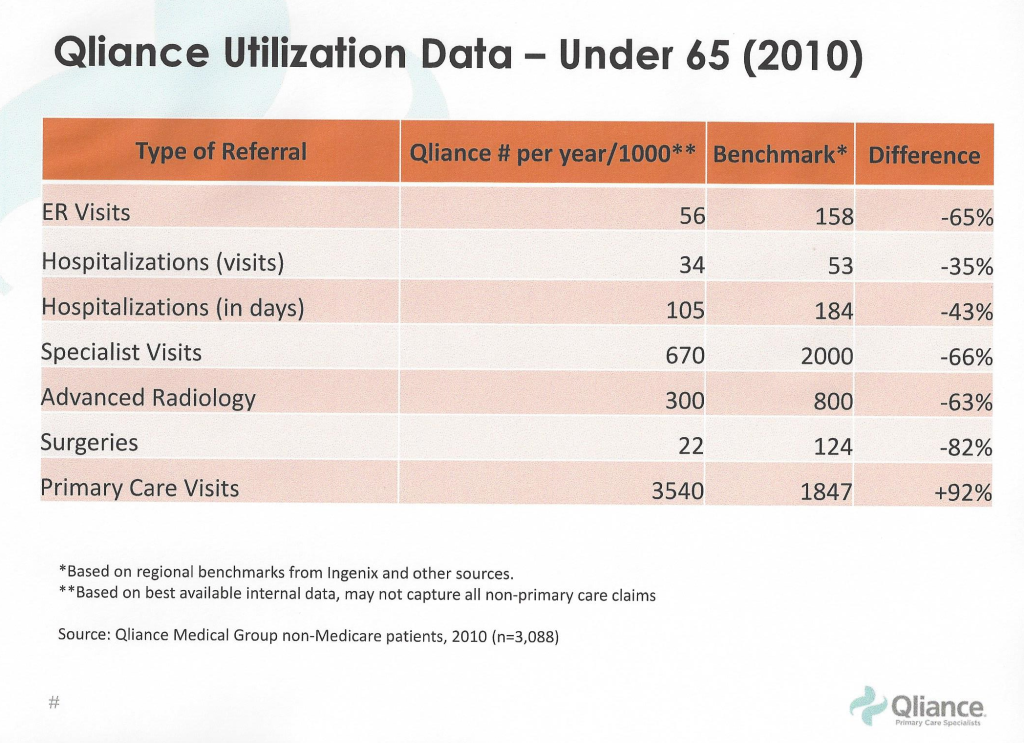
First, one of the main benefits of the direct primary care model is physicians have more time to spend with their patients to actually figure out what is wrong and treat problems appropriately; and therefore, they need to refer patients less often. As family physicians, I believe we are well trained to handle the myriad of problems that patients may present with, but we do not have enough time to adequately address them in a 10 minute office visit, so we often feel compelled to refer them to specialists. QIiance has demonstrated that when you have the time to spend with patient, specialist and ER visits, surgeries and hospitalizations are all significantly reduced
Media from QlianceMedia from Qliance
Second, even specialists are willing to reduce their fees when they are guaranteed payments in a more timely manner. Again, when we eliminate the insurance middleman, we significantly reduce the uncertainty and/or time it takes to pay for services. In reality, fees for sub-specialty visits, services, surgeries, etc. are set for insurance companies who routinely underpay by a significant amount, since they can negotiate much lower payments. Again, if we could eliminate the “insurance bureaucracy tax” by reducing administrative costs through the removal of the insurance middle man, specialists could charge patients much less for the actual services they provide.
MARBLEHEAD — Direct Primary Care is a concept based on the idea that physicians should be dedicated to their patients, and care for them based on their needs, not their insurance plan, says Dr. Jeffrey Gold.
The concept strives on building strong patient/physician relationships and eliminating third parties, such as insurance companies, for primary care.
Many believe it’s a solution to a lot of the problems we see in the primary health care system: waiting time, high costs, and not understanding treatments. Gold is one.
“Let’s get back to using health insurance for what insurance should be used for: the big things, the unexpected things, surgeries,” said Dr. Jeffrey Gold of Gold Direct Care in Marblehead, “not the day-to-day primary care which is expected and what people need.”
Instead, DPC offices charge a fixed monthly rate and provide patients with unlimited doctor visits and unlimited time during each visit. Doctors spend more time with patients and are able to provide a wider variety of care so that most procedures can be performed in the office, Gold says.
When a patient does need to be referred to a specialist, DPC doctors communicate extensively with the specialists in order to ensure the best care for the patient. “When I do refer out, I have a much better dialogue with the specialist,” said Gold.
“I have better referrals, because I’m not referring as many people out and I can communicate with the specialist because I have more time,” he said. “This results in better care for the patient, which is the ultimate goal and should be the ultimate goal.
“This is getting back to what medicine is supposed to be about, which is the patient and physician relationship,” said Gold. “The doctors in the program are trying to provide quality care but the current system doesn’t allow it.”
This method is an attempt to stray away from the traditional medical system, which Gold says has become more about “how many people you can see rather than the quality of the care.”
“Our goal is to help the patient,” he said. “It’s difficult when you’re in a room seeing 20 people a day. That’s not why I went to school for so long.”
Gold aims to have about 750 patients as opposed to the 2,500 he had when working in traditional medicine. The purpose, he said, is “for the patient to really have a lot of questions and be more engaged with their health. I have the opportunity to do that.
“It’s gratifying to spend time with people that you genuinely care about and make sure they are getting what that they need,” he said.
While DCP does not involve insurance directly, a membership does not take the place of insurance. It’s important to know that you still need insurance for emergency situations and surgeries.
“DCP is not insurance, it’s a service.” Gold said.
“All primary care services are included under that fee. I can still take care of someone who doesn’t have insurance but I would never encourage someone to not have insurance. We recommend a high deductible plan so that you’re covered in all aspects of your care.
“We’re trying to work with insurance companies to get the right plan for people. Get them higher quality care,” he said.
While eliminating insurance all together is not recommended, the idea behind DCP is to remove it at the primary care level.
“I work like a gym membership; people can use it or not use it but they’ve paid for the service,” he said.
“Patients pay “a monthly age-based fee that pretty much encompasses 99 percent of what I do in the office,” he said. Falling under the remaining one percent are things like blood work, routine women’s health screenings and even house calls, which Gold says range between $3-$30.
According to Gold, there are many added benefits of being a patient of a DPC office. Doctors have 24/7 availability. They give patients their cell phone number, giving them the option to call, text, email, FaceTime and skype.
“I can talk to a patient on the phone from the comfort of their own bed,” said Gold.
For Gold, it’s about changing the experience patients have with health care.
“Nobody wants to go to the doctor and we’re trying to change that,” he said “It’s up to us to try to fix this and make it better and the only way to do that is to think outside the box and make things simpler.
“It allows for people to have a say in what they’re getting and how they’re getting it,” he said “I hope we get to the place where people demand better and get better.”
“No more copays, no more pesky insurance cards and more time to ask your doctor important questions. This is the vision of Marblehead doctor Jeffrey Gold, the first physician in Massachusetts to open a Direct Primary Care practice.
Direct Primary Care is a model of healthcare in which patients pay the doctor a flat-rate, monthly or annual fee for a range of medical care and services. Dr. Gold’s patients will pay a monthly, age-based fee ranging from $30 to $125, which includes an annual physical exam, according to Marketwired.“
 I am writing this as a sincere thank you to the Research Team and Incite Health at the Center for Primary Care at Harvard Medical School for taking the time to visit us this summer to see and hear what Direct Primary Care is all about (Here is link to story: Harvard Medical School Team Visits Gold Direct Care). If an institution of Harvard Medical Schools caliber can get behind this model of care, the potential for growth and implementation is boundless. Hopefully, we showed their team that the simplistic model of Direct Primary Care in combination with an appropriate high deductible/Health Savings Account insurance plan accomplishes everything that the Quadruple Aim is about:
I am writing this as a sincere thank you to the Research Team and Incite Health at the Center for Primary Care at Harvard Medical School for taking the time to visit us this summer to see and hear what Direct Primary Care is all about (Here is link to story: Harvard Medical School Team Visits Gold Direct Care). If an institution of Harvard Medical Schools caliber can get behind this model of care, the potential for growth and implementation is boundless. Hopefully, we showed their team that the simplistic model of Direct Primary Care in combination with an appropriate high deductible/Health Savings Account insurance plan accomplishes everything that the Quadruple Aim is about: